

YOUR SPECIALIST
DR. MICHAEL DANIELAK
DDS, Cert. Pros, FRCD(C)
Board Certified Prosthodontist
Dr. Michael Danielak is a certified specialist in prosthodontics and is a Fellow of the Royal College of Dentists of Canada. He serves as a Clinical Assistant Professor of Health Science in the Restorative Dentistry Department at the University at Buffalo, state of New York, teaching prosthodontic residents in the dental school clinic one day per week. Dr. Danielak also teaches two seminar-style courses after hours to train the specialty residents in digital dental technology and DSLR dental photography.
READ MORE
Following his prosthodontics residency, Dr. Danielak completed another year and a half of fellowship training devoted to the surgical placement and restoration of implants at the University at Buffalo, School of Dental Medicine in the state of New York. Upon returning to Canada, Dr. Danielak successfully challenged the Canadian prosthodontics specialty boards to become a board certified prosthodontist.
Dr. Danielak has a calm and compassionate demeanour when interacting with his patients. He has experience treating patients with a range of intra-oral conditions from simple to complex in order to restore function and aesthetics. It would be his pleasure to consult with you regarding your prosthetic dental needs.
WHAT IS A PROSTHODONTIST?
The field of prosthodontics is one of nine of the recognized dental specialties by the Canadian Dental Association. Prosthodontists are considered the experts in dentistry when it comes to the diagnosis of advanced dental problems and treatment planning for reconstructions. Identification of the cause of oral deterioration is a key element to any dental treatment in order to stop the progression of disease, minimize its impact, develop an effective treatment strategy, and lower the chance of future recurrence of disease.
WHY DO I NEED A PROSTHODONTIST?
Many dental problems can be corrected by a general dentist, such as crowns or fillings on a few teeth. However, more complex cases involving the entire set of teeth or complex bite issues often requires a coordinated approach employing the expertise of perhaps several different dental or medical specialists.
The role of Prosthodontists in these cases is two-fold: They not only administer professional care to the patient, but they also coordinate and oversee the dental team in a patient’s treatment plan. They will develop the overall treatment plan and synchronize treatment sequences with other specialists as well as with general dentists in order to provide the most comprehensive care.
PROSTHODONTIC SERVICES
Our patients can be confident that they receive a full range of treatment options during their consultation. At Cedar Pointe Prosthodontics, our goal is to provide a comfortable, patient-centered approach, ethical options, timely treatment, and excellent outcomes for all our patients. Informed consent is our highest priority, and we ensure that before you commit to treatment, you have been made aware of your intra-oral condition, treatment options, the proposed treatment sequence, treatment timing, and the financial commitment. For additional information on the range of treatment options and services available for you, please contact the office.
Crown, Bridge, Veneers
Implant Solutions
Digital Dentistry
Extraction & Bone Grafting
Sedation
nitrous oxide (laughing gas), oral sedation (sleeping pill)
Dentures
Full Mouth Reconstruction
tooth-borne, implant-borne, fixed, removable, all-on-X, all-on-4
Treatment of Abnormalities
BEFORE & AFTER
See examples of Dr. Danielak’s work from several of his patients.




Complete Dentures
This patient presented with ill-fitting complete dentures and was concerned that the “orange colour” of the acrylic from her current prostheses made her teeth look fake when she smiled. To ameliorate her concern, clear bases were processed to blend in with the supporting tissues and internal characterization was used before secondary processing to give the tissue portion more depth and colour. The patient left satisfied with the improved function and aesthetics of the new removable complete dentures.







Short Teeth Due to Altered Passive Eruption
This patient presented with moderate wear of the anterior dentition and mild- to moderate-dental fluorosis. Her chief concern was primarily aesthetic in nature regarding the “short” look of her front teeth and the discolorations. Treatment involved opening of the vertical dimension to re-gain restorative space, crown lengthening in the maxillary anterior, and restoration with all-ceramic bonded crowns and onlays in the maxilla. Long-term provisionals were used to verify aesthetics and function prior to fabrication and delivery of the definitive restorations.The mandibular arch remained largely unrestored due to 12 months of pre-prosthetic orthodontics for alignment of the teeth, space distribution, and levelling of the occlusal plane.







Short Teeth Due to Tooth Wear
This patient presented with a severe occlusal disharmony, supra-eruption of the posterior teeth, moderate wear of the anterior dentition, a tilted occlusal plane, and residual ridge atrophy in both width and height.Treatment involved bone grafting and posterior implant placement, opening of the vertical dimension, and restoration with bonded all-ceramic restorations in the maxillary and mandibular anterior teeth. The natural posterior teeth did not require re-restoration. Function, aesthetics, and correction of the tilted occlusal plane was verified first utilizing long-term provisionals, and accepted by the patient, before the definitive restorations were fabricated.

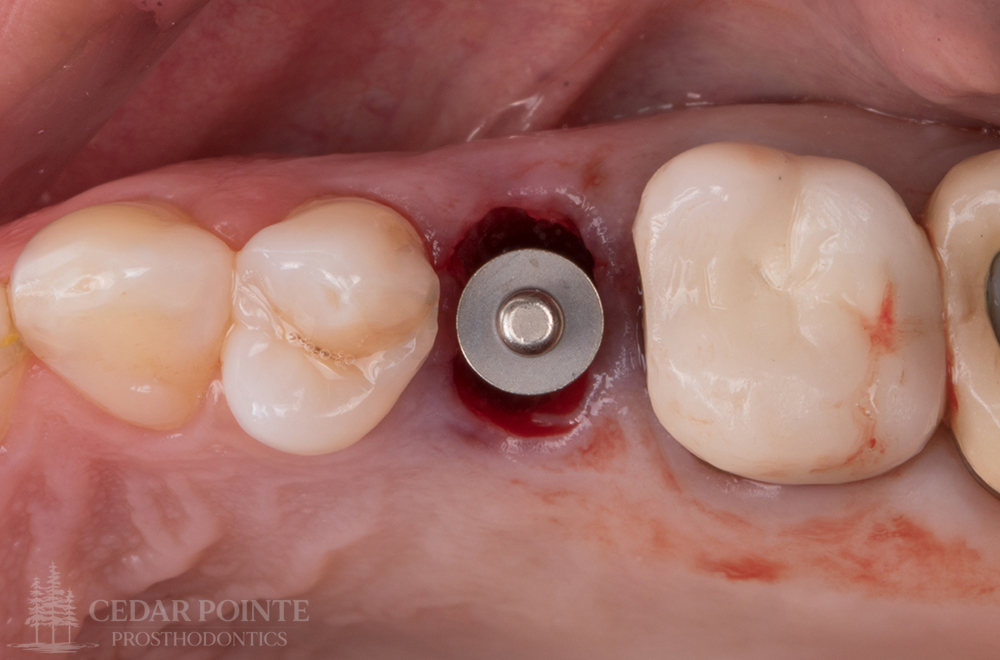


Immediate Implants
Often times when teeth become non-restorable due to cavities or fractures, a treatment option is to extract the remaining tooth root and place an implant immediately into the residual socket. This typically reduces the total treatment time by 3-4 months and allows patients to receive the final implant crown much faster after only 4-5 months of total treatment time. Careful case selection is critical though, as not all failed teeth can undergo with type of immediate implant treatment.
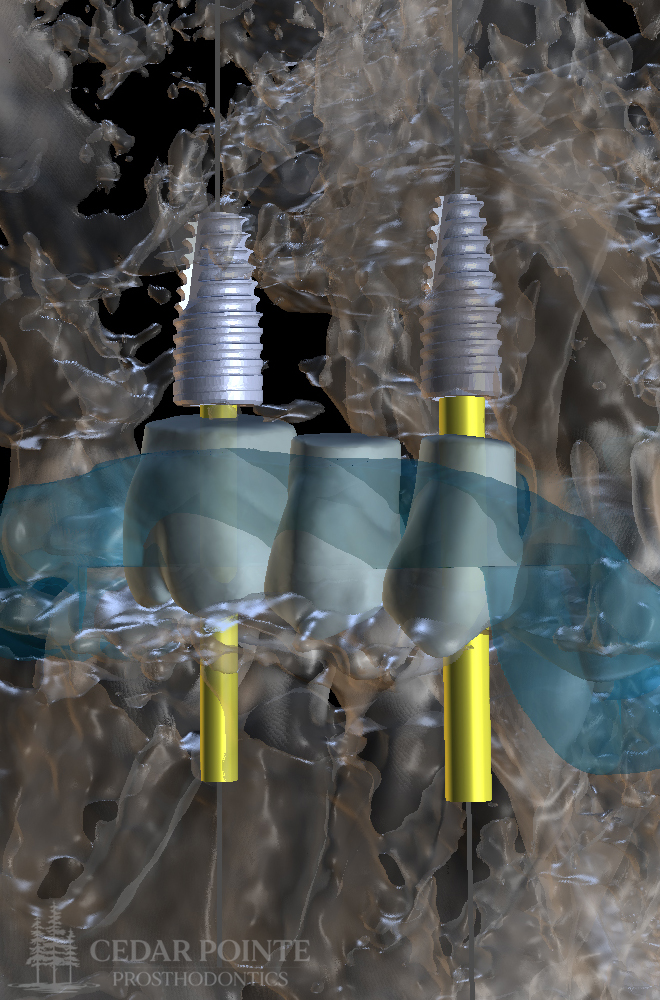


Digital Implant Planning
My preferred diagnostic imaging modality of choice for the majority of my implant cases is a 3D CBCT scan. This scan can be performed in-office and provides 3D cross-sectional information of the proposed surgical site(s). Conventional 2D imaging techniques often don’t provide enough information and leaves some room for error or “guesswork” during surgery which is not ideal. Surgical workflows are determined on a case-by-case basis and utilize either standard placement protocols or a fully-guided workflow.




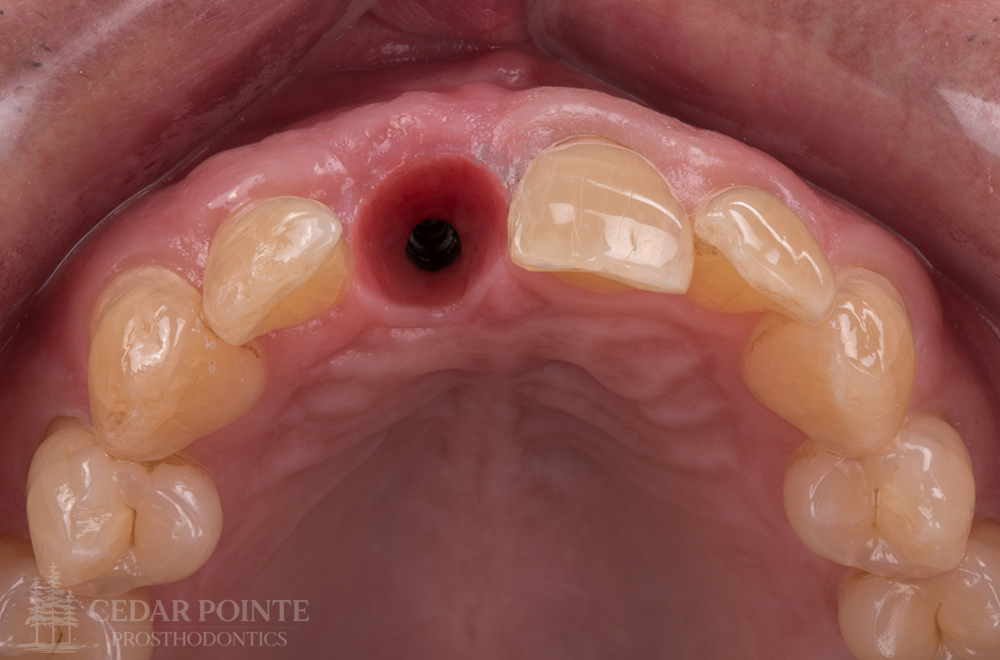
Anterior Implants
Treatment planning implants in the anterior aesthetic zone begins with a full aesthetic and functional evaluation. In this region, implant depth plays a large part in the overall aesthetic success of the final prosthesis. Additional time is spent to plan anterior cases to ensure the final position of the implant will have the correct vertical depth, using a diagnostic wax-up as the reference. Emergence profiles can become compromised if implants are placed too shallow.


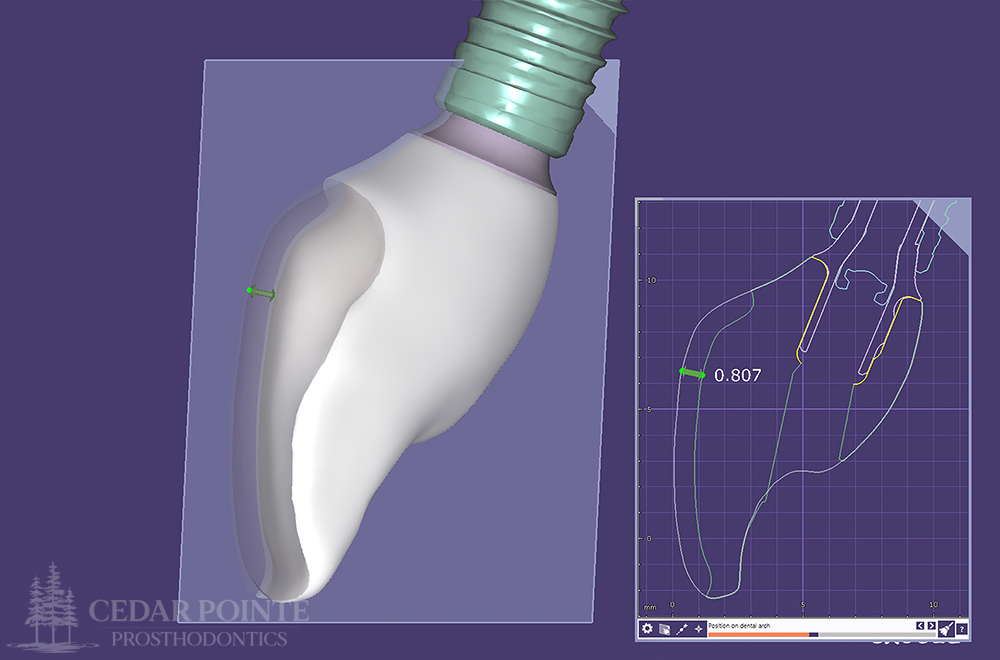

Anterior Implants
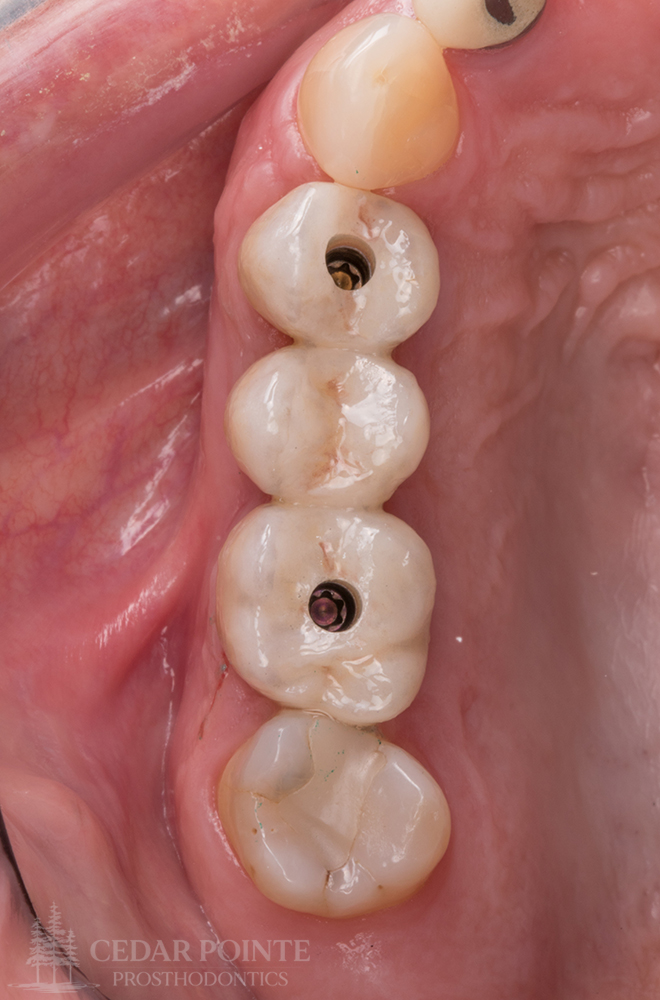
I highly prefer screw-retained implant restorations over cement-retained. While screw-retained implant restorations are more technique-sensitive and do require slightly more chair time during initial delivery, their ease of retrievability during maintenance visits, as well as the absence of residual cement remaining in the sulcus, are tremendously advantageous for improved long-term outcomes, making them my primary restoration design of choice.






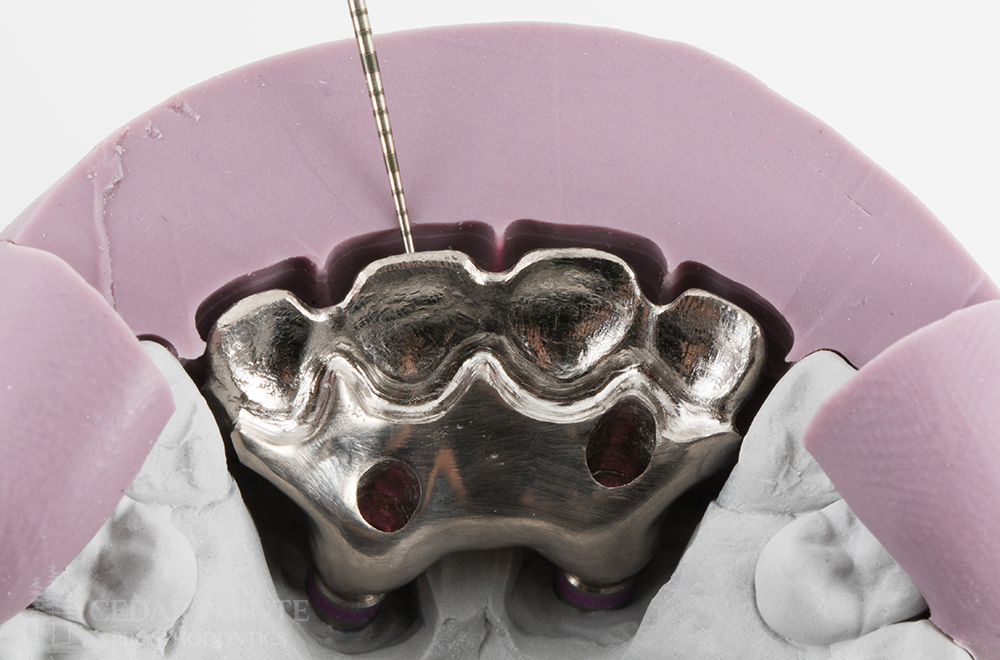
Implant Complication Management
This patient presented with advanced bone loss in the maxillary anterior due to a complex history of trauma in the region, as well as two failed implants. The lack of adequate bone width and tissue in the region are believed to be the etiologies of implant failure. Due to the large vertical restorative space, the restoration of choice was a one-piece porcelain-fused-to-metal casting. The casting was designed with enough cut-back of the metal to ensure a uniform thickness of porcelain layering. As with all aesthetic cases, a long-term implant provisional was used to drive the design of the definitive restoration.


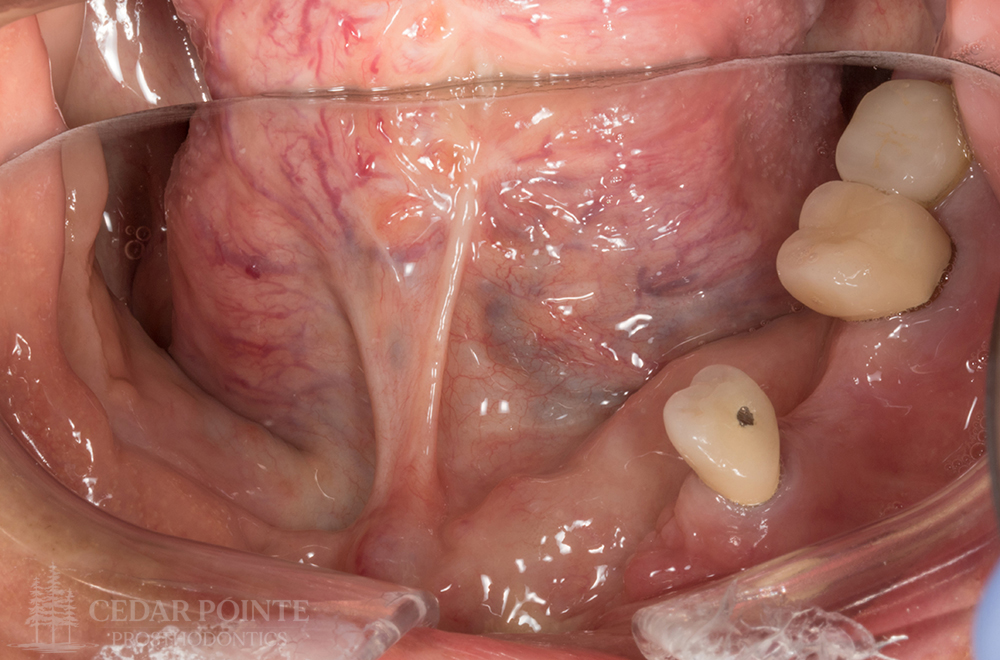




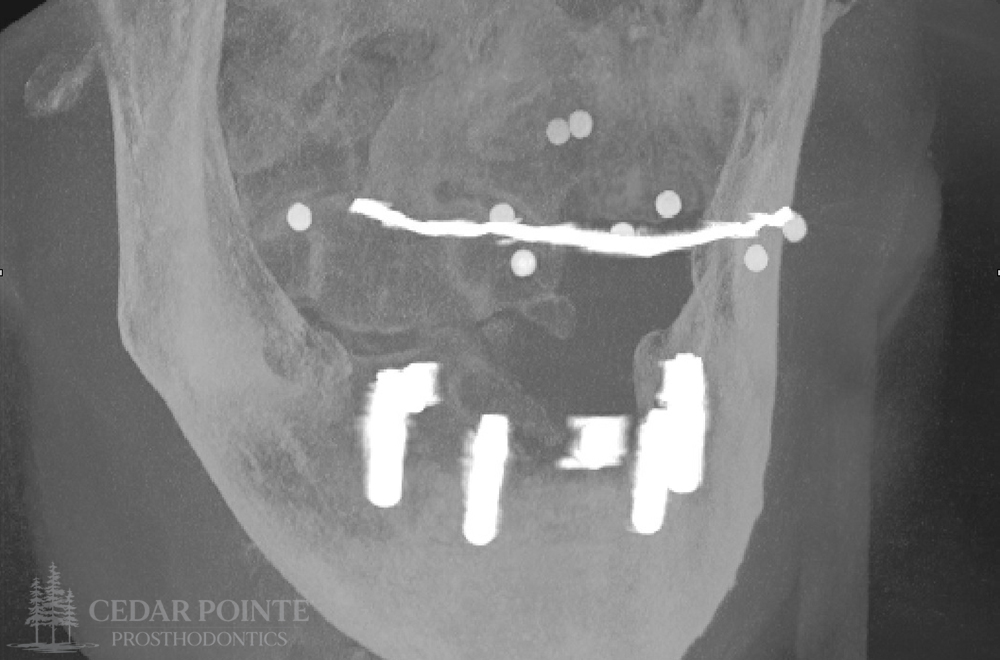
Complex Trauma
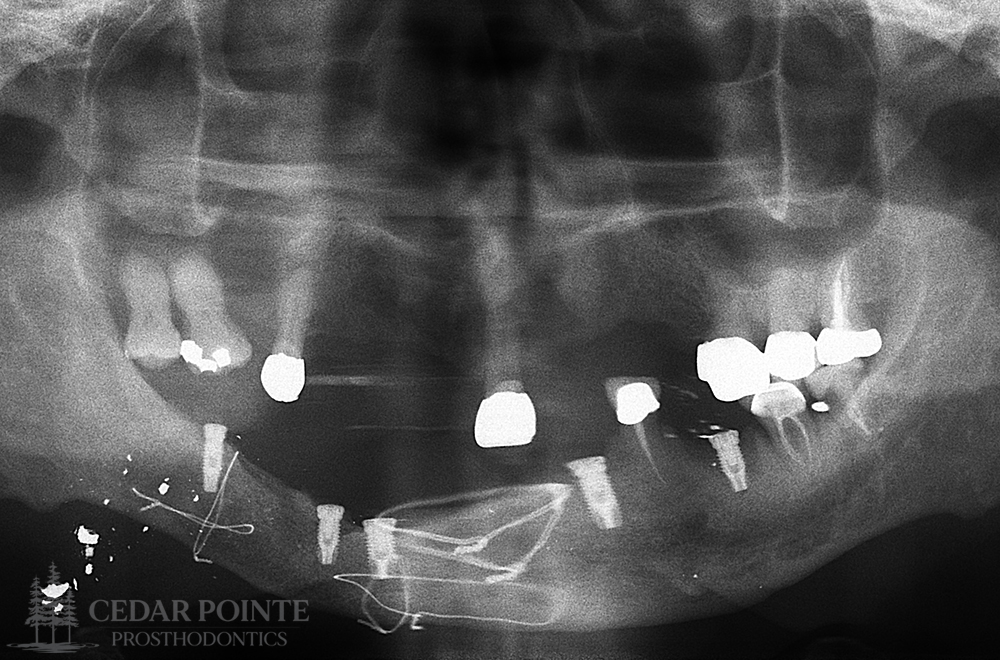
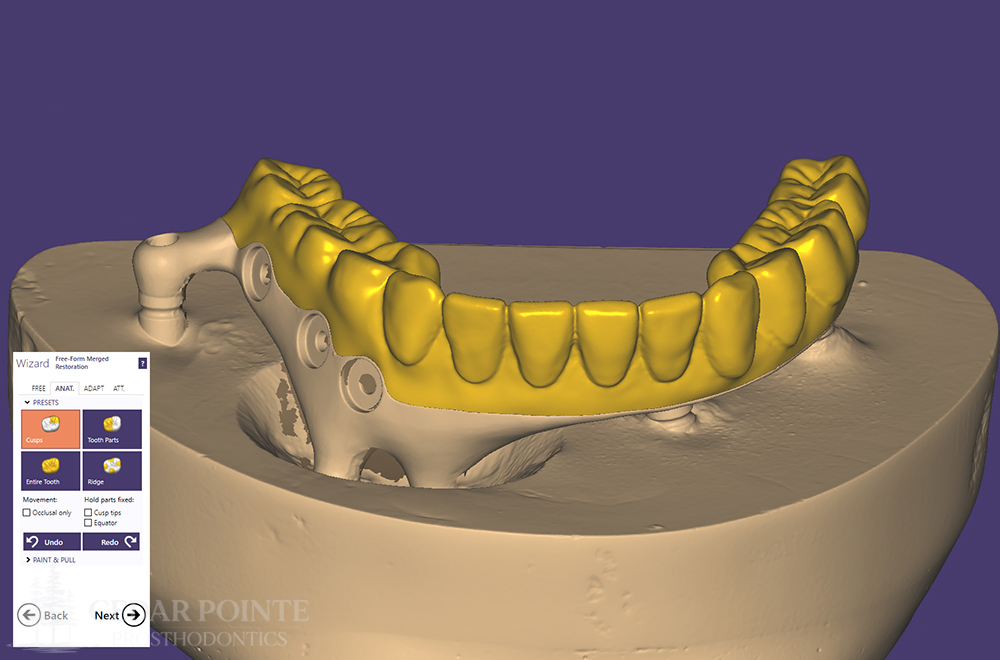
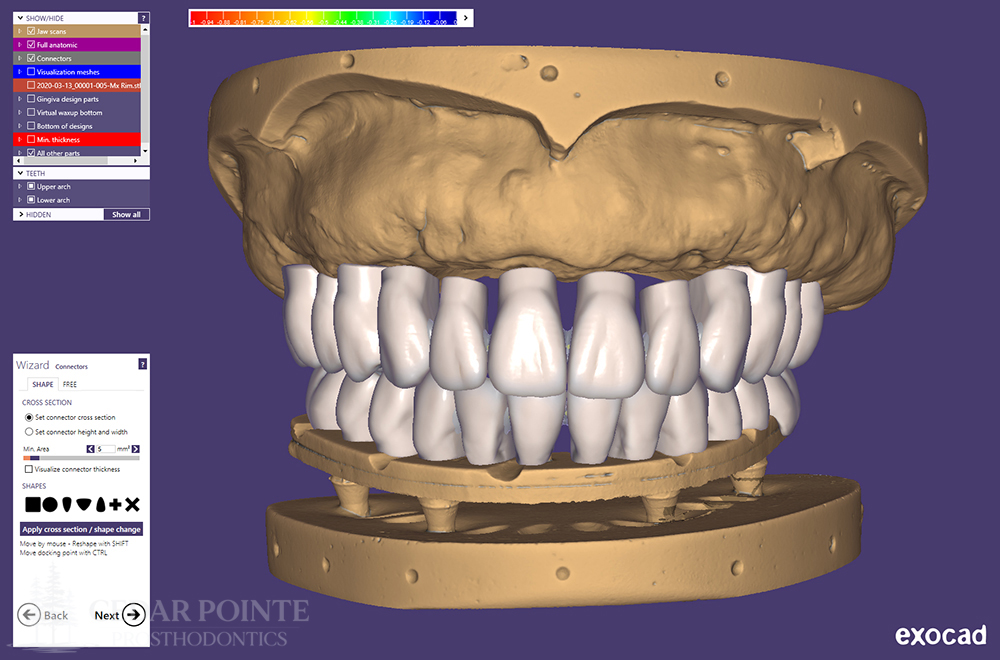
This patient suffered a gunshot injury to the right mandible during the Vietnam War. At the time of injury, a fibular graft was used to repair the mandible and a skin graft was used to repair and close the soft tissue. The patient had functioned adequately with a removable prosthesis for years, until the loss of an essential support tooth. He requested a fixed option at this point due to imminent loss of the remaining failing teeth in the mandible. Five implants were placed, and a CAD-CAM milled titanium bar substructure with milled acrylic teeth was designed for the superstructure. This design was unique in that a magnetic removable lip plumper was designed to fit onto the right side of the prosthesis to improve lip and cheek tonicity during speech due to a significant neuromuscular deficit as a result of the original injury.








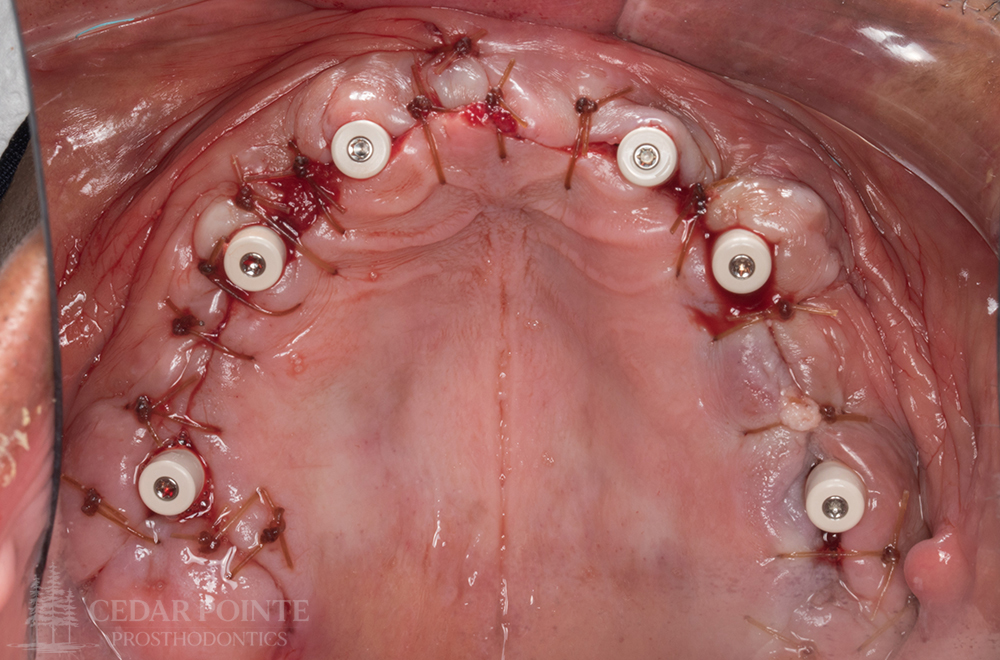
Full-Arch Implant Rehabilitations
When patients present with a failing dentition, a reasonable treatment option is to convert to a fixed or removable implant-supported prosthesis. While this increases both treatment time and the financial commitment, implant-borne prostheses have been shown to have a higher long-term survival rate versus compromised, heavily restored teeth with a poor or guarded prognosis. Several factors are considered when determining the best type of implant-supported prosthesis to provide for a patient. Restorative space, aesthetic demand, functional capacity, patient ability and dexterity, and financial capability, must be considered during initial treatment planning.

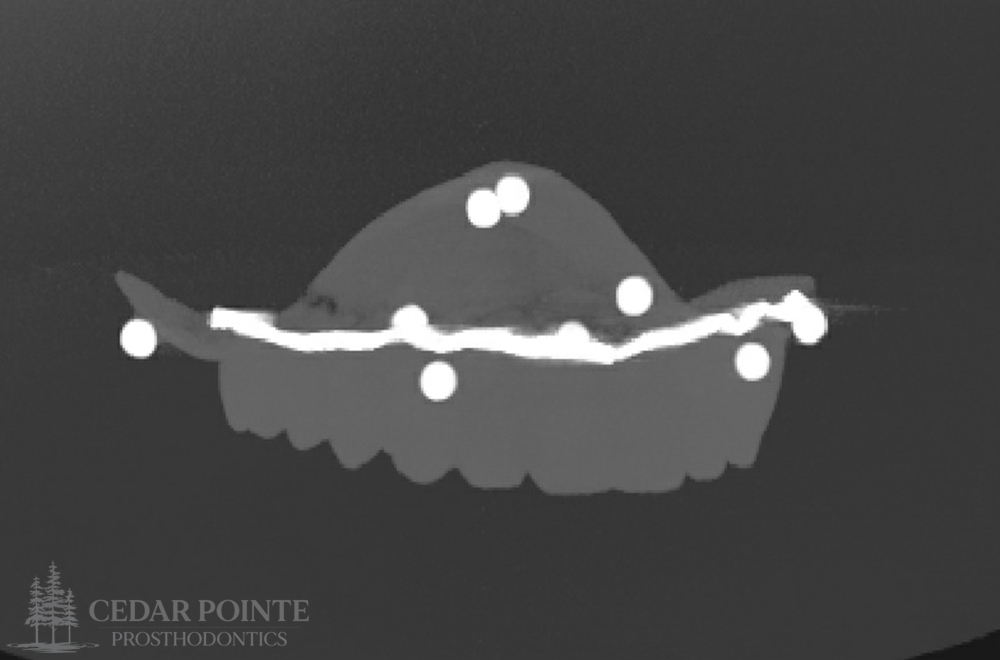
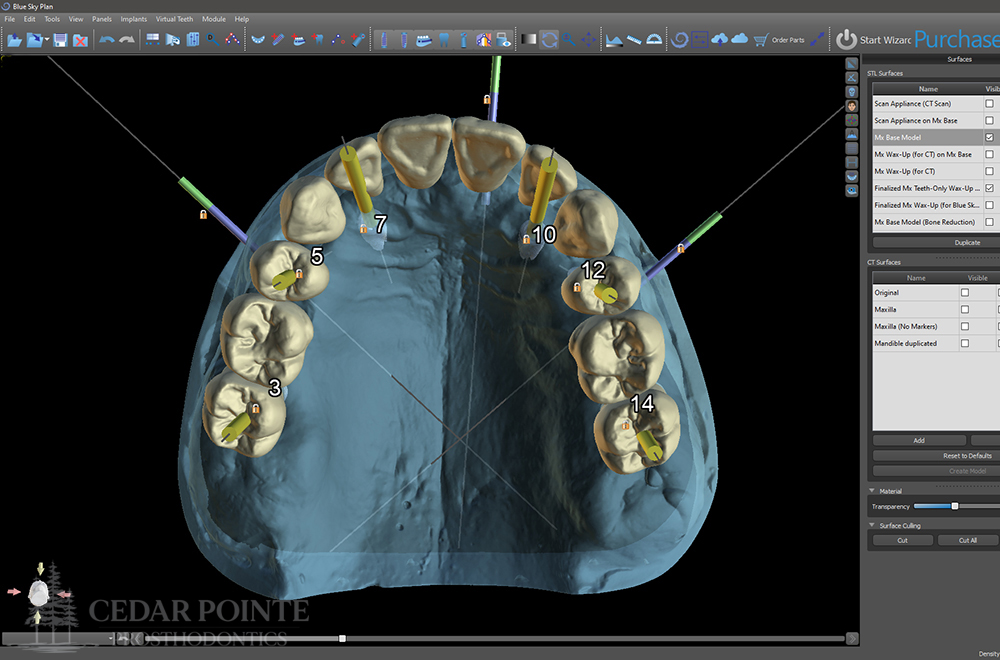




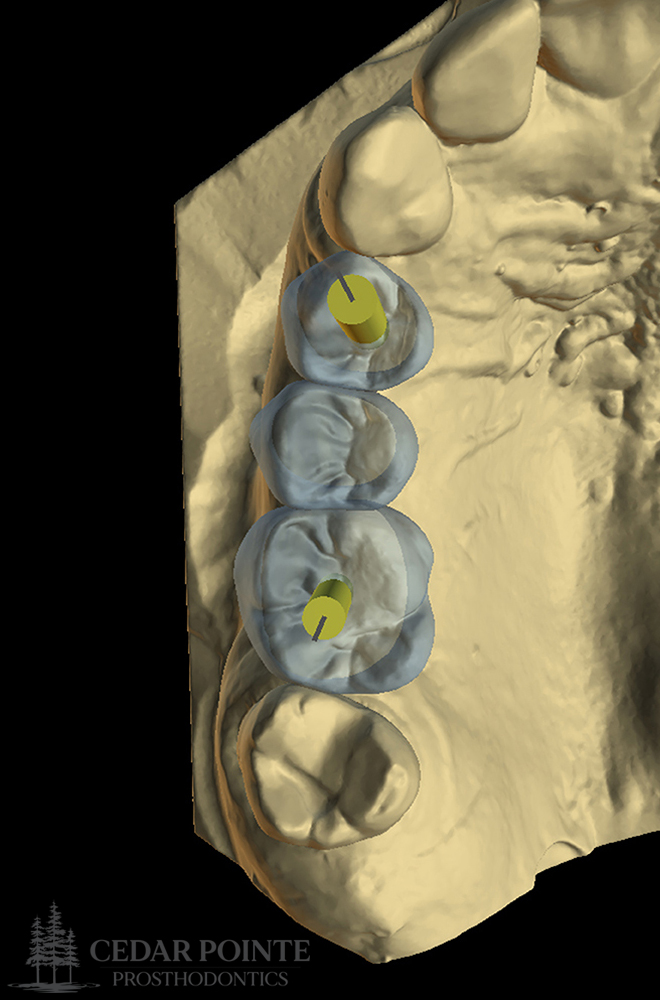
Prosthetically-Driven Fully-Guided Surgery
Advanced full-arch cases involving both surgical and restorative treatment require meticulous treatment planning and collaboration to ensure proper execution during the treatment stage and a satisfactory end result. My preference for these types of cases is the use of prosthetically-driven digital planning and a fully-guided surgical workflow. These guides ensure that implants are placed true to the planned location and leave very little room for error, especially when proximity to anatomical structures is a concern. Prosthetically-driven implant planning also allows implant screw channels to be located centrally within occlusal surfaces of posterior teeth and on the lingual surfaces of anterior teeth where they are hidden from view.
REFERRALS & FORMS
Cedar Pointe Prosthodontics is accepting new patients and referrals from general dentists and dental specialists for specialty prosthetic care. If you do not currently have a general dentist but would like to be seen, please phone the office to set up a consultation appointment with Dr. Danielak.
If you are a general dentist or dental specialist and would like to refer a patient to the office, please download the fillable referral form, fill out the requested information (electronically or by print), and e-mail or fax it back to the office. Please include as much pertinent information as you can.